
Heartburn is usually a sign of acid reflux
The stomach is protected from the acid that it produces but the esophagus can be injured by acid that refluxes up from the stomach.
Fortunately, there are defences in place that prevent acid from harming the esophagus.
Fortunately, there are defences in place that prevent acid from harming the esophagus.
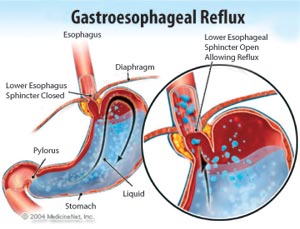
At the end of esophagus, there is a group of muscles that are called the lower esophageal sphincter (LES).
The job of the lower esophageal sphincter is to relax when we swallow to allow food to pass into the stomach but to then close tightly to prevent food and acid from regurgitating back into the esophagus.
Heartburn or acid reflux occurs when the LES either transiently or permanently does not close tightly.
The job of the lower esophageal sphincter is to relax when we swallow to allow food to pass into the stomach but to then close tightly to prevent food and acid from regurgitating back into the esophagus.
Heartburn or acid reflux occurs when the LES either transiently or permanently does not close tightly.
Transient relaxations can occur spontaneously or with certain foods such as coffee, alcohol, and chocolate. Large meals can create stomach pressure that overwhelms the LES.
Patients with transient relaxations have heartburn infrequently.
People with transient relaxations are easily treated with topical antacids such as TUMS, Rolaids, Maalox or Gaviscon that quickly buffer the acid in the esophagus rendering it harmless.
Patients with transient relaxations have heartburn infrequently.
People with transient relaxations are easily treated with topical antacids such as TUMS, Rolaids, Maalox or Gaviscon that quickly buffer the acid in the esophagus rendering it harmless.
People with permanent dysfunction of the lower esophageal sphincter will suffer from heartburn and regurgitation on a regular basis.
Patient with heartburn 2-3 times per week often benefit more from medications that decrease acid production rather than just buffer the acid.
There are 2 major groups of antacids: Histamine 2 receptor antagonists and Proton pump inhibitors
Patient with heartburn 2-3 times per week often benefit more from medications that decrease acid production rather than just buffer the acid.
There are 2 major groups of antacids: Histamine 2 receptor antagonists and Proton pump inhibitors
Antacids
|
Histamine 2 receptor antagonists (H2RA) decrease the acid production in the stomach by blocking the histamine 2 receptor. Common H2RA are cimetidine (Tagamet), famotidine (Pepcid) and ranitidine (Zantac).
|
Proton pump inhibitors (PPI) block the acid production more profoundly than the H2RA. Common PPI are omeprazole (Losec), esomeprazole (Nexium), pantoprazole (Pantaloc), lanzoprazole (Prevacid), rabeprazole (Pariet) and dexlanoprazole (Dexilant)
|
Lifestyle changes
Some people can successfully resolve their heartburn symptoms with certain lifestyle changes.
- Avoiding trigger foods (coffee, alcohol, citrus fruits, chocolate, spices)
- eating smaller, more frequent meals
- raising the head pf the bed 15-20 cm to prevent night time reflux
- stop smoking
- lose weight
Hiatal hernia
|
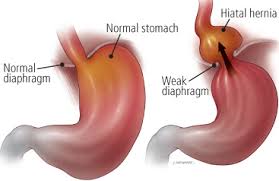
A hiatal hernia occurs when part of the stomach pushes up into the chest above the diaphragm through a loosening of the diaphragm opening. This also causes a breakdown in the defence against reflux.
A person with a hiatal hernia will often complain of heartburn and regurgitation. Since food may sit in the hernia before it passes into the rest of the stomach, they may feel full more quickly. |
|
Is heartburn ever caused by other things than acid reflux?
Heartburn is a sensation caused when the nervous system controlling the esophagus is irritated.
Acid reflux is the most common irritant but there are others.
Some people are sensitive to acidic foods such as lemons or oranges that give symptoms of heartburn. Others may react to bile or other stomach fluids that have regurgitated into the esophagus. Smoking is a common irritant.
An infection of the esophagus (usually in people with a poor immune system) or a cancer of the esophagus can also give symptoms of heartburn.
Acid reflux is the most common irritant but there are others.
Some people are sensitive to acidic foods such as lemons or oranges that give symptoms of heartburn. Others may react to bile or other stomach fluids that have regurgitated into the esophagus. Smoking is a common irritant.
An infection of the esophagus (usually in people with a poor immune system) or a cancer of the esophagus can also give symptoms of heartburn.
Should I be checked with a gastroscopy?Most patients have simple acid reflux that is easily treated with medications or lifestyle changes. Since there is no worry of complications there is no need to investigate. However, the following groups of people should have a gastroscopy.
|
1. Patients over the age of 50 with new onset heartburn 2. Patients over the age of 40 with at least a 5 years of regular acid reflux (to assess for Barrett's esophagus) 3. Patients not adequately treated with PPI twice daily 4. Patients with any alarming symptom such as swallowing difficulties, blood loss, weight loss, vomiting or anemia |
For how long should I take my medications?
For patients with chronic acid reflux, I first recommend taking the prescribed antacids, either the H2RA or the PPI, for at least 2-3 months. This gives enough time for the esophagus to heal and its sensitivity to reduce. After that, I recommend trying to stop it and seeing if or when the symptoms will return. This will allow you to use the least amount of medications to keep you comfortable.
Can acid reflux lead to cancer?
|
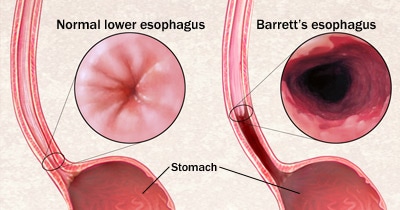
It can unfortunately but it is rare. The cancer related to acid reflux is called esophageal adenocarcinoma.
Acid damage to the esophagus over a period of many years can cause the lining of the esophagus to change. This lining change is called Barrett's esophagus. This is the first step that is present before cancer develops. Barrett's esophagus is detected by performing a gastroscopy. People with Barrett's esophagus are then screened every 3 years for further cell changes called dysplasia that may increase the risk for cancer further. |
|